|
Evidence-based scientific responses to Jeanne Bergman
re House of Numbers By: Eleni Papadopulos-Eleopulos, Valendar F. Turner, John M Papadimitriou, David Causer
INTRODUCTION We agree with Bergman that scientific answers must be based on “evidence-based science”. In science there are no fake questions – only fake answers. Bergman’s “answers” to the questions raised in House of Numbers consist of proclamations without one iota of “evidence-based science” to back her up. Hence, by her own definition, her answers are fake. We remind Bergman: 1. Scientists are obliged to deny nothing and question everything. The “legitimate scientist” and Nobel laureate Jacques Monod: “In science, self-satisfaction is death. Personal self-satisfaction is the death of the scientist. Collective self-satisfaction is the death of the research. It is restlessness, anxiety, dissatisfaction, agony of mind that nourish science”. Perter Abelard: The first key to wisdom is assiduous and frequent questioning…For by doubting we come to inquiry, and by inquiry we arrive at truth”. Neither is there “incontrovertible evidence” for anything in science. Richard Feynmann: “Scientific knowledge is a body of statements of varying degrees of certainty – some most unsure, some nearly sure, none absolutely certain”. 2. Scientists respond when challenged. Howard Temin, the father of modern retrovirology: “when an experiment is challenged no matter who it is challenged by, it’s your responsibility to check. That is an ironclad rule of science, that when you publish something you are responsible for it…even the most senior professor, if challenged by the lowliest technician or graduate student, is required to treat them seriously and consider their criticisms. It is one of the most fundamental aspects of science” (emphasis in original).1 HIV scientists do not respond to challenges. In fact, according to the rules at AIDSTruth, “We will not engage in any public or private debate with AIDS denialists or respond to requests from journalists who overtly support AIDS denialist causes”. Apparently these “legitimate scientists” cannot stick to their own rules. For over a quarter of a century the Perth Group has denied nothing but questioned every aspect of the HIV theory of AIDS. In our scientific publications, including peer-reviewed publications, we have raised many questions but virtually no HIV expert has responded. In order to draw attention to the problematic nature of the HIV theory of AIDS we published many papers with questions included in the text or titles. These include the following: 1. Papadopulos-Eleopulos E. Reappraisal of AIDS: Is the oxidation caused by the risk factors the primary cause? Med Hypotheses 1988;25:151-162. http://www.theperthgroup.com/SCIPAPERS/reappraisalofaids.html 2. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM. Is a positive Western blot proof of HIV infection? Biotechnology 1993;11:696-707. http://www.theperthgroup.com/SCIPAPERS/biotek8.html 3. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Causer D. The Isolation of HIV: Has it really been achieved? Continuum 1996;4:1s-24s. http://www.theperthgroup.com/CONTINUUM/pgvsduesbergreward.html 4. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Causer D, Page BA. HIV antibody tests and viral load – more unanswered questions and a further plea for clarification. Curr Med Res Opinion 1998;14:185-6. http://www.theperthgroup.com/SCIPAPERS/furtherplea.html 5. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Stewart G, Causer D. HIV antibodies: further questions and a plea for clarification. Curr Med Res Opinion 1997;13:627-34. http://www.theperthgroup.com/SCIPAPERS/epcurmedres97.html 6. Papadopulos-Eleopulos E, Page BA, Causer D, Turner VF, Papadimitriou JM, Alfonso H. Would Montagnier please clarify whether HIV or oxidation by the risk factors is the primary cause of AIDS? Med Hypotheses 2006;67:666-8. http://theperthgroup.com/SCIPAPERS/PGMontOSMH2006.pdf 7. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Page BA, Causer D, Alfonso H et al. A critique of the Montagnier evidence for the HIV/AIDS hypothesis. Med Hypotheses 2004;63:597-601. http://www.theperthgroup.com/SCIPAPERS/MHMONT.pdf 8. Turner VF. Reducing agents and AIDS – Why are we waiting? Med J Aust 1990;153:502. http://www.theperthgroup.com/SCIPAPERS/RedAgent.pdf 9. Turner VF. The HIV Western blot. Med J Aust 1994;160:807-808. http://www.theperthgroup.com/SCIPAPERS/VFTDax.pdf Still no response. Apart from publications we also put questions directly to many HIV/AIDS experts, including John Moore. Almost without exception none have responded. In 2006 we emailed John Moore with several questions and a request for a dialogue. He wrote back: 24th September 2006 - Turner, You have gone through 21 drafts and a considerable amount of effort to say absolutely nothing that is of any conceivable interest to me. I’m glad you wasted your time though, as communicating with me (or trying to) is harmless, compared to the damage you AIDS denialists do to innocent people you attempt to confuse and thereby cause to be harmed. So, continue to knock yourself out, so to speak. All you will receive from me is my continued contempt, and derision. John Moore. (It was not 21 drafts. It was 2 drafts. John Moore was not familiar with the way MS Word saves files attached to emails that are returned with the same file name. Furthermore, we are not AIDS denialists). 26th September 2006 - You are confusing me for someone who is interested in what you have to say, and you are confusing yourself for someone who merits a more detailed response. Kindly correct yourself of those delusional tendencies. I despise you and your fellow AIDS denialists, and I regard your level of “scientific analysis” as pitiful and laughable. One expert, Luc Montagnier, did not respond although he promised to do so on more than one occasion. At the beginning of the AIDS era one of us (EPE) wrote a paper entitled Reappraisal of AIDS: Is the oxidation caused by the risk factors the primary cause? After two rejections by Nature in 1986 it was published in 1988 in Medical Hypotheses.2 In 1991 a few of our papers including our Medical Hypotheses paper was sent to Montagnier who promised he would study it and come back to us with his comments. http://theperthgroup.com/VARIOUS/MontagniertoEPE1Oct1991.jpg He did not come back to us. In 1990 the journal Research in Immunology, a Pasteur Institute publication, opened its “columns to Dr P Duesberg and Dr L Montagnier, who have agreed to discuss the matter of whether HIV is the causative agent of AIDS” and “invited other contributions on this topic”. In our contribution entitled “Oxidative Stress, HIV and AIDS” we wrote “As long ago as 1983, one of us (E.P.-E.) proposed that oxidative mechanisms are of critical significance in the genesis of AIDS (acquired immune deficiency syndrome). A prediction of this hypothesis was that the mechanisms responsible for AIDS could be reversed by the administration of reducing agents, especially those containing sulphydryl groups (SH groups). The discovery of HIV resulted in a broadening of this hypothesis in that it considered oxidative stress as a principal mechanism in both the development of AIDS and expression of HIV”.3 In the same contribution as well as earlier4 we presented evidence that cellular activation is an oxidative phenomenon.” Montagnier may have agreed to discuss matter but failed to do so, either with us or Peter Duesberg. However, to our surprise, nine years after the publication of the oxidative theory, six years after he received our papers and five after our Research in Immunology publication, Montagnier and his colleagues published a paper in which they wrote “In AIDS pathogenesis, oxidative stress is proposed as a metabolic alteration that favours disease progression by inducing both viral replication and apoptotic death...Indeed, the evidence that oxidative stress induces, while antioxidants inhibit, HIV replication and apoptosis suggests the use of these molecules as an antiretroviral therapy to reduce cell death in AIDS patients”5 (italics ours). When we read Montagnier’s book “Virus”, published in 2000,6 and his presentation to the European Parliament in 2003,7 we published a letter in Medical Hypotheses entitled “Would Montagnier please clarify whether HIV or oxidation by the risk factors is the primary cause of AIDS?”.8 Montagnier never responded. SPECIFIC RESPONSES Bergman: But Leung is an HIV denialist—he has said he is “neutral” on the issue of HIV/AIDS, which means he rejects the evidence-based science that has conclusively proved the existence of HIV and its causative role in AIDS, a fatal disease syndrome. Neutral does not mean non-acceptance. A journalist, making a film, presenting points of view, is not there to proselytise. He makes no judgment either way because his personal views are neither the subject nor the issue. His job is to present all sides, ask questions and make the viewer think. All HIV experts including Robert Gallo and the Nobel committee accept that the “evidence-based science” for the existence of HIV was published by Montagnier et al in an historical paper published in 1983 entitled Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). In keeping with the title of Montagnier’s seminal paper, all “HIV” experts, including Montagnier, claim the existence of “HIV” has been proven by a procedure known as “virus isolation”. Yet few “scientists, doctors and advocates”, much less laypersons, are aware that in virology the word “isolation” is devoid of its everyday meaning. The Perth Group has polled clinicians, non-scientist professionals and laypersons asking each what he or she understands by the title of Montagnier’s paper. As one would expect all give a description of an object obtained on its own separate from all other objects. Furthermore, it is a given that only objects that exist can be isolated. In other words, “isolation” = existence. Fait accompli. “Isolation”, which is derived from the Latin “insulatis”, means “made into an island”. Either wittingly or unwittingly, but at great convenience, this word has been misappropriated by virologists to the point where it almost qualifies as spin. Ex cathedra pronouncements, announcements or statements that “HIV” has been “isolated” are accepted by virtually everyone as proof of the existence of a unique retrovirus without raising a single question of veracity. However, when the rare individual does probe the oratory, the “HIV” experts are loath to elucidate. This is well exemplified in the House of Numbers by Leung’s interviews with David Baltimore and Robin Weiss: “I [Leung] asked Nobel Laureate Dr. David Baltimore and Dr. Robin Weiss how they would isolate and photograph this elusive virus”. Baltimore answered “Well, didn’t Dr. Gallo do that [isolate the virus]? I mean he actually isolated it, so...I mean, why should I do all of this? This is all text book stuff you are asking me...I don’t want to be your text book, you know? I got other things to do.” According to Bergman, at the time of this interview Baltimore did not know he was being “deceived” and believed he was participating in a film that would inform and educate the general public about “HIV” and AIDS. Yet, in regard to his refusal to explain isolation, all Bergman could say is “He [Baltimore] is reasonably annoyed that this guy [Leung] is asking him how he would personally isolate the virus”. Neither was Robin Weiss forthcoming: “I am not quite sure what is behind your question about isolation”. What was “behind it” was an attempt by Leung to discover what “evidence-based science” proves “HIV” exists. To inform his viewers about what actual experiments retrovirologists have done in their laboratories to prove there is such an entity as “HIV”. Why did Baltimore and Weiss refuse to respond to this most reasonable request? Why did they decline to explain, for the benefit of viewers, this seminal data? Is virus “isolation” so arcane or sacrosanct it cannot be spoken? Is that why Baltimore was “reasonably annoyed”? Baltimore refuses to enlighten Leung with the reply virus “isolation” “is all text book stuff”. Which text book and what stuff? It is impossible to find a satisfactory definition of isolation anywhere in the virological literature, including in virology text books”.9-11 In regard to “HIV”, by “isolation” Montagnier means the detection of an enzyme activity, reverse transcriptase activity (RT), in two consecutive cell cultures. However, such a definition, the measurement of an enzyme activity, can only mean detection of a retrovirus, and then if and only if RT is specific to retroviruses. Which it is not (see below). Nowadays most often “HIV” isolation means the detection of a protein in a cell culture using an antibody. On this basis performing a pregnancy test on a blood sample is “isolation” of the placenta. Thus it is little wonder neither Baltimore nor Weiss want to talk about it. The fact is that in the case of all “HIV” experts and all papers published on “HIV isolation”, “HIV” “isolation” is not isolation. Nonetheless, whatever it is virologists claim is “isolation” in terms of proving the existence of a virus, they, like everyone else, including Montagnier and Gallo (see below), accept that, in order to determine the biochemical constituents of a virus, the virus particles must first be isolated=separated=purified from the cells in which it is cultured. Why? Because viruses and cells are made of the same stuff. Distinguishing between viral proteins and nucleic acids and cellular proteins and nucleic acids is an absolute requirement in order to establish what is viral and what is cellular. Especially given the use of viral proteins and nucleic acids as reagents for diagnostic tests. If a scientist does not know which proteins and nucleic acids are viral and which are cellular he will never know what he is testing for. In the 26 years since the “discovery” of “HIV” no scientist has presented evidence for this elementary step—the purification of “HIV”. To the contrary, all the evidence proves none of the taxonomically distinct particles all said to be one and the same retrovirus, “HIV”, have been purified.12,13 Hence there is no “evidence-based science” whatsoever for the existence of “HIV” proteins or nucleic acids and thus “HIV” and “HIV” tests. What follows is a summary of Montagnier’s experiments as described in his “Isolation” paper from 1983. Bergman can judge for herself whether Montagnier’s evidence for the “isolation” and hence the existence of “HIV” has any substance.14-17 1. Lymphocytes from a patient at risk of AIDS (BRU) were cultured with many chemical agents and then transferred to another culture which contained lymphocytes from a healthy blood donor mixed with the same chemicals. In both cultures Montagnier and his colleagues detected reverse transcriptase activity. They claimed detection of RT in the BRU culture proved BRU was infected with a retrovirus and the finding of RT in the co-culture proof the BRU retrovirus was transmitted to the healthy blood donor cells. However, as far back as 1973, the first and second authors of the Montagnier paper knew that RT is not specific to retroviruses and can be found in normal, uninfected cells.18 “This enzymatic activity [RT] can be explained by the presence of some virus particles in these regions [sucrose density bands other than 1.16 g/ml], and since similar polymerase activity has been found in normal cells, may be mainly ascribed to the cellular enzyme”.18 In other words, 10 years before they made their claim, they knew it had nothing to do with “evidence-based science”. At present, knowledge of the non-specificity of RT is so widespread it has even appeared in the popular press, in material read by people contemplating investment in biotechnology stocks.19 2. The supernatant fluid from the co-culture was added to a culture of umbilical cord blood lymphocytes. In this culture they found RT and particles bearing some of the morphological characteristics of retroviruses, “typical type-C” particles. They claimed this proved the retrovirus from BRU was transmitted to the umbilical cord lymphocytes. However, in 1983 every retrovirologist (Montagnier and the first and second authors of the 1983 paper are retrovirologists), must have known that type-C particles are found in nearly all normal human placentas20 and budding retroviral-like particles are a feature of cultured, umbilical cord lymphocytes.21 In other words, Montagnier et al’s claims had nothing to do with “evidence-based science”. 3. Montagnier claimed the particles visualised in the umbilical cord culture were retrovirus particles because, in a sucrose density gradient, they banded at the density of 1.16 g/ml. “That this new isolate was a retrovirus was further indicated by its density in sucrose gradient, which was 1.16 [g/ml]”. In fact they claimed the 1.16 g/ml band was “purified, labeled virus”. That is, it contained nothing else but retroviral-like particles. This claim was made despite the absence of any electron microscopic data and hence proof that the banded material Montagnier called “purified” virus contained particles of any kind, retroviral, non-retroviral, pure or impure. Montagnier later justified this particular claim on the basis that “we published in Science (May 1983) a [sucrose density] gradient which showed that the RT had exactly the density of 1.16. So one had a peak which was RT. So one has fulfilled this criterion for purification”.22 In other words, not only did Montagnier regard RT as proof for isolation and transmission of “HIV”, he also regarded detection of this enzyme activity in a density gradient as proof for purification of “HIV”. This bizarre conclusion is the basis of the “incontrovertible evidence” for the “overwhelming scientific consensus” that HIV exists and is the cause of AIDS”. When BRU’s serum (antibodies) was added to the proteins in the 1.16g/ml band three proteins were found to react - p25, p45 and p80. They did not provide any additional information on p80 but it was not designated an “HIV” protein. p45 was said to be cellular and p25, now known as p24, and the antibodies which reacted with it, to be “HIV”. Because the p25 (p24) protein did not react with antibodies directed against the retrovirus HTLV-I p24 protein, Montagnier claimed he had discovered a new human retrovirus. One should note that since Montagnier discovered only one “HIV” protein, p24, not only had he discovered a new retrovirus, he had also discovered the world’s first (and only) “one protein” retrovirus. One does not have to be a scientist to realise that if two out of the three proteins present in “purified” virus are not “HIV” then the 1.16 g/ml band cannot be “purified” virus. If two proteins are not “HIV” then why is the third? And on what basis are the antibodies which reacted with p24 “HIV”, while those that reacted with p45 and p80 not “HIV”? The scientific truth came to light in 1997 during an en camera interview Montagnier gave to the French investigative journalist Djamel Tahi. In response to the question “But there comes a point when one must do the characterisation of the virus. This means: what are the proteins of which it’s composed?”, Montagnier replied: “analysis of the proteins of the virus demands mass production and purification. It is necessary to do that”. Yet in response to further questioning he admitted he and his colleagues did not purify HIV. “I repeat we did not purify”.22 The minimum absolutely necessary but definitely not sufficient condition for Montagnier to claim his solo p24 protein is an “HIV” protein is to have proof for the existence of at least some particles with the morphology typical of retroviruses in the 1.16 g/ml banded material. Montagnier did not publish electron micrographic images of the “purified” virus hence, during the same interview, he was asked why not. His answer was stunning. He said that in the “purified” virus, even after a “Roman effort”, Charles Dauget, the Pasteur Institute electron microscopist, was unable to find any particles with “the morphology typical of retroviruses”. Much less purified particles of any morphology. In a subsequent interview with the same journalist Charles Dauget himself confirmed that the “purified labeled virus” consisted of cellular debris. There were no retroviral particles at all in the “purified” virus (DT personal communication). This is as good “evidence-based science” as one can get that Montagnier and his colleagues never had proof for a retrovirus in any of their cultures or the patient BRU. And the most specific “HIV” protein, p24, is nothing more than a cellular protein. In 1986 Robert Gallo claimed he had presented “clear cut”23 evidence that HIV is the cause of AIDS in four papers published in Science in May 1984. This claim has been accepted by HIV experts including Montagnier (sometimes) and Bergman. The HIV theory of AIDS states: HIV infection to T4 cell destruction to clinical syndrome to death. To assert such a claim Gallo must have evidence which proves: 1. The existence of HIV. 2. HIV kills the T4 cells. 3. HIV is present in all AIDS patients. 4. T4 decrease is both necessary and sufficient to cause the appearance of the AIDS indicator diseases. To prove the existence of “HIV” Gallo relied on the same phenomena as Montagnier. That is, RT, particles visualised in the cell culture and reactions between the proteins in the 1.16 g/ml band, which he also called “purified” virus, and antibodies in patient sera. However, as far back as 1976 Gallo knew that particles with the morphology of retroviruses are not necessarily retroviruses, even if they contain RT. “Release of virus-like particles morphologically and biochemically [with RT] resembling type-C virus but apparently lacking the ability to replicate have been frequently observed from leukaemic tissue”.24 There were two main differences between Gallo’s and Montagnier’s experiments: (a) Gallo used an immortal cell line, HUT78 (H9) in place of umbilical cord lymphocytes. The HUT78/H9 cell line originated in a patient with leukaemia. According to Montagnier this type of cell line contains “a real soup” of retroviruses.22 (b) Gallo tested more patients. In a 2007 court case Gallo acknowledged that, to identify the proteins and the RNA of a new retrovirus, one must purify the retroviral particles. “You have to purify”.25 During the same court case Gallo was asked: “In his [Montagnier’s] 1983 Science paper he referred to the 1.16 band as the purified virus. Is this right?” Gallo answered “He did a 1.16 cross [sucrose] – gradient in that paper, yes. I don’t know if he said it was purified. If you do that you don’t have much virus” [page 1300]. Like Montagnier, Gallo claimed the 1.16 g/ml band was “purified” retroviral particles but also like Montagnier published no electron microscopic data—neither in 1984 nor at any other time. In court he stated: “A sucrose gradient barely purifies”.25 If banding in density gradients “barely purifies”, and in the 1.16 g/ml band “you don’t have much virus” why (a) did Gallo use the density gradient banding to purify “HIV”; (b) did he call the 1.16 g/ml “purified virus”?; (c) were the two proteins, p24 and p41, which reacted with antibodies in patient sera, said to be “HIV” proteins and the antibodies “HIV” antibodies? Since both Gallo and Montagnier agree purification is necessary to prove the existence of a new retrovirus and Gallo did not know “if he [Montagnier] said it was purified”, why did Gallo (a) recommend the publication of Montagnier’s paper; (b) submit his own papers for publication? Notwithstanding, Gallo reported the “isolation” of “HIV” from 37% of AIDS patients and that 88% had antibodies that reacted with proteins in the 1.16 g/ml band, the “purified” virus, using either the ELISA or Western blot. However, at that time even the HIV experts accepted the specificity of the ELISA was very low. The criteria used for a positive WB was a reaction with p41, a protein which, according to Montagnier and other researchers12 from the AIDS Vaccine Program, SAIC, National Cancer Institute-Frederick Cancer Research and Development Center, Frederick, Maryland, is the ubiquitous cellular protein actin.16 Most importantly, in none of the four Gallo papers is there any attempt to prove HIV kills the T4 cells, much less that a decrease in T4 cells (immune deficiency, AID) is the cause of the diseases from which AIDS patients die. Obviously, if one bases one’s opinion on “evidence-based science” one has no choice but to conclude in 1984 Gallo did not prove HIV causes AIDS. In January 1986 Montagnier wrote the “...cytopathic effect of LAV [“HIV”] can ONLY be observed in activated T4 cells” (emphasis added). In the same year Gallo and his associates reported experiments where they prepared T-cell cultures (which contained 34% T4 cells), from normal donors. Cultures were stimulated with PHA and then (i) “infected” with “HIV”; (ii) left uninfected. Control cultures remained both unstimulated and uninfected. After 2 days of culture the proportion of T4 cells in the stimulated-uninfected and stimulated-infected cultures was 28% and 30% respectively, while at 6 days the number was 10% and 3%; the controls not changing significantly. Thus, stimulation is sufficient to cause a decrease in T4 cells while “infection” with “HIV” makes no significant difference. Furthermore, the quintessential part of this experiment went unreported. That is, data from the “infected” but unstimulated cell cultures. However, they did write “the expression of HTLV-III [“HIV”] was always preceded by the initiation of interleukin-2 secretion, both of which occurred only when T-cells were immunologically [PHA] activated. Thus, the immunological stimulation that was required for IL-2 secretion also induced viral expression, which led to cell death”.26 Hence by 1986 Montagnier and Gallo were in agreement that: 1. “HIV” by itself → no T4 destruction. 2. “HIV” plus stimulation → T4 cell destruction; 3. Stimulation by itself → T4 cell destruction. In other words, in the 1980s Montagnier and Gallo showed that “HIV” is not sufficient for a decrease in T4 cells. And Gallo’s evidence shows that in the presence of antigenic stimulation (activation), which is typical and intense in AIDS patients, it is not even necessary. Yet, for more than 20 years all of Bergman’s “legitimate scientists, doctors and advocates” led the world to believe that “HIV” is the cause of the immune deficiency and the clinical AIDS syndrome. Bergman: “House of Numbers” asks if there is really a scientific consensus about HIV/AIDS. The real answer is: YES. There is an overwhelming scientific consensus, based on incontrovertible evidence, that HIV exists and is the cause of AIDS. “Overwhelming scientific consensus” is the mantra of every “HIV” protagonist. Daniel Kuritzke’s recent posting at www.houseofnumbers.org/Kuritzkes__Statement.html is no exception. The origin of the “HIV” theory lies with a handful of scientists who claim to have proven the existence of a new retrovirus in 1983/84. This claim, without which there cannot be a retroviral theory of AIDS, has been accepted by virtually all scientists and doctors despite the fact few know the details or could defend the theory. The only thing “overwhelming” about the “overwhelming consensus” is the “overwhelming” numbers of “scientists, doctors and advocates” who accept and support it. It appears as if Bergmann and the Perth Group read different scientific journals. In 2008 Montagnier was awarded the Nobel Prize in Physiology or Medicine for his historical paper published in Science, May 1983 for proving the existence of HIV. In 2003, in the New England Journal of Medicine,27 Gallo and Montagnier wrote: “In early 1983, a clear-cut isolate [“HIV”] was obtained in Paris...”. Yet in 1984 Gallo, writing in Science, stated that Montagnier’s evidence did not prove “true isolation” of HIV.28 In 1997 Goudsmit29 wrote: “The BRU lymph node was first cultured in early January 1983 and, on January 15, it shed an enzyme absolutely unique [sic] to the lentivirus group...The BRU virus grew slowly and with difficulty, but its identity and activity were reported in the May 20, 1983 issue of Science...The Pasteur Group was widely acclaimed but very worried. In the world of virology, finding a new virus is not enough: You must propagate and isolate the organism for analysis by other virologists. The French had not yet isolated their new lentivirus”.29 In 2009 Vahlne,30 published a paper in Retrovirology in which he stated “Regarding whom should get the credit for the discovery of HIV, this review should enable the reader to come to his or her own conclusion. Mine, however, is different from that of those of my fellow faculty members that presently make up the Nobel Committee for the Nobel Prize in Physiology or Medicine...In reality, in my view there is no evidence whatsoever in this paper [Montagnier’s 1983 Science paper] that a new human retrovirus has been isolated!” Since Vahlne’s paper was promptly posted at AIDSTruth.org, we assume the “legitimate scientists, doctors and advocates” at AIDSTruth agree with his analysis. Needless to say, when the Perth Group submitted a response to Vahlne’s paper, it was rejected by Retrovirology. Is this the overwhelming consensus for the discovery of the virus that has killed 25 million people? In 1988 Gallo and Montagnier wrote: “after two weeks of culture, reverse-transcriptase activity was detected in the culture medium. A retrovirus was present”.31 In 2002 Montagnier wrote: “Fifteen days later, Françoise Sinoussi (by then Barré-Sinoussi) found the first traces of RT in the supernatant of the lymphocyte culture, indicating the presence of a retrovirus”. However, as mentioned above, according to Barré-Sinoussi and Chermann, the first and second authors of the 1983 Science paper, the “evidence based science” as far back as 1973 showed that RT activity does not indicate a retrovirus. “This enzymatic activity [RT] can be explained by the presence of some virus particles in these regions [sucrose density bands other than 1.16 g/ml], and since similar polymerase activity has been found in normal cells, may be mainly ascribed to the cellular enzyme”.18 This was confirmed by Gallo in 1976: “Many laboratories subsequently reported the detection of reverse transcriptase in extracts from normal cells”.32 Gallo and his colleagues themselves reported: “An endogenous and completely RNA-dependent...DNA polymerase [reverse transcriptase] activity was obtained from leukemic blood lymphocytes (and myeloblasts) and from PHA stimulated (but not in unstimulated) normal human blood lymphocytes”.33 Harold Varmus agrees. “...reverse transcription is hardly unique to retroviruses; it is now recognized as a widespread phenomenon in eukaryotic cells”.34; “evidence has made it clear that reverse transcription takes place...in the uninfected cells of yeast, insects and mammals”.35 Is this more scientific consensus? In his 1983 paper Montagnier said that his retroviral particle were “typical type-C”. In 2007, in a court case Gallo stated, “...although I am a co-author, I contributed really nothing to that paper. It was Gonda that recognised the lenti/retrovirus nature, not me. He corrected a mistake from lack of the structural familiarity by almost all retrovirologists with this family known by veterinarians. That is the answer. Montagnier, of course, did not know”. He also pointed out that HIV is a lentivirus “it is clear even by its genomic analysis”. Gallo’s testimony, page 1307.25 Commenting on the paper by Gonda and Gallo36 Montagnier, in his 2000 book Virus, wrote: “Science published an article by his [Gallo’s] group that showed similarities of sequences between HTLV-I, -II, and –III, and then, more curiously, between these and the lentivirus prototype, the Visna sheep virus. The two sets of findings proved entirely false, and nothing from these two articles holds any longer. We were beginning to seriously wonder whether Science was not starting to compete with the Journal of Irreproducible Results! The Pasteur team, to clear the matter up, also unraveled the Visna virus sequence in record time...there was no significant homology (similarity) between the Visna and LAV [“HIV”] sequences”.6 Elsewhere in the same book Montagnier referred to his experimental evidence that Visna and LAV were also biologically different: “But then the horse virus [a lentivirus] refused to grow in human lymphocytes, and our virus [“HIV”] would not grow in horse lymphocytes. Moreover, neither the horse virus not the Visna sheep virus would attack T4 lymphocytes or cause immunosuppression”. The one electron micrograph Montagnier showed of “HIV” during his Nobel lecture has barely any of the principal morphological features of retroviruses, much less, a lentivirus.37 The question then is: what is the “evidence-based science” which led the “legitimate scientists, doctors and advocates”, including Montagnier and Gallo, to conclude “HIV” is a lentivirus? What exactly is the “evidence-based science” upon which the consensus on the lentiviral nature of “HIV” is based? The “HIV” experts cannot agree even how many knobs are present on the surface of the “HIV” virus particle. These are the knobs which, according to the “legitimate scientists, doctors and advocates”, are a MUST for infectivity. No knobs=no infection. In Virus, Montagnier wrote: “Particles of HIV are shaped like little spheres, each with roughly 80 rounded projections shaped like pegs”. In the 2005 textbook38 co-authored by Niel Constantine (who appears in the House of Numbers) and Professor Elizabeth Dax, Head of the Australian National Serology Laboratory and International Expert on HIV testing, there are “72 knobs or spikes of the external envelope of HIV”. According to Hans Gelderblom and John Moore, immediately after being released from the cell membrane “HIV particles” possess an average of 0.5 knob per particle which are rapidly lost, but also pointed out that “it was possible that structures resembling knobs might be observed even when there was no gp120 [knobs] present, i.e. false positives”.39 That is, there may not be any knobs. In 2003 Kuznetsov and his colleagues40 reported a study utilising atomic force microscopy that contradicted what all “HIV” experts claim. They reported that “The clusters of gp120 do not form spikes on the surface of the HIV as is commonly described in the literature. The clusters are hardly protrusions at all. We suggest that spikes, knobs, observed by negative-staining electron microscopy may be an artifact of the penetration of heavy metal stain between envelope proteins. Indeed, the term “spike” appears to have assumed a rather imprecise, possibly misleading definition, and might best be used with caution”. In other words, this posits zero knobs on the so-called “HIV” particle. Hence the “evidence-based” scientific consensus has knob counts for the “HIV” particle of 80, 72, 0.5 (on average), possibly zero and actually zero. Of interest is the picture at the very top of the AIDSTruth homepage. Presumably the custodians of the AIDSTruth website believe this image lends weight to the existence of “HIV” on the basis of the particles illustrated in the image. This is a scanning electron microscope (SEM) picture which has been colour enhanced using a computer (retroviral particles and cells are not green or red). The image does not include its source (patient, type of culture, scientific paper) and does not have a size bar. Without a size bar (or the magnification) the most fundamental property of retroviral particles, the diameter, cannot be determined. By design the SEM is suited for the study of surface features, not internal structures of particles and cells. However, without knowledge of the presence or absence of a core and its morphology, as well as other internal morphological features, it is not possible to claim these particles have even the appearance of a retrovirus. The resolution is low and for this reason it is also not possible to determine whether the particles do or do not have knobs. One would have thought the scientists at AIDSTruth would have posted the best possible image in support of the virus that has killed “over 25 million people worldwide”. No professional electron microscopist would release the image at AIDSTruth. AIDSTruth is not alone. At its website “Focus on the HIV/AIDS Connection” the National Institutes of Allergy and Infectious Diseases present their evidence “Why is there overwhelming scientific consensus that HIV causes AIDS?”. The answer to this “consensus” includes an invitation to visit http://www.virology.net/Big_Virology/BVretro.html in order to see “Electron micrographs and other images of HIV”. Of these 25 images the majority are diagrams, artists’ renditions or computer graphics. Only eight images are electron microscopic pictures and none identify the source or nature of the material portrayed. Significantly, none has a size bar, that is, in no EM is it possible to determine the dimensions of the particles or other morphological features. Publishing electron-micrographs of “the retrovirus HIV” devoid of the requisite morphologies features of a lentivirus is not confined to AIDSTruth or the NIAID. On 20th November 2003 Nature published a news item entitled “Medical journal [BMJ] under attack as dissenters seize AIDS platform”. This one page article includes a scanning electron micrograph with a caption which reads “The BMJ’s website carries postings that deny that HIV, seen here in [sic] a white blood cell, causes AIDS”. This bizarre image, resembling a spoonful of overflowing spaghetti, occupies some 22% of the available space, which presumably reflects its importance. However, the source of the electron micrograph is not given, there is no size bar, there are no labels and the magnification is not specified. The appearance of the cell in the micrograph is unlike any white blood cell that has ever traversed the vascular system. If the particles displayed are indeed a retrovirus they are obviously on the cell and not in the cell as the author claims. Moreover, these surface particles are cylindrical, not spherical, and are several microns in length. Such appearances and dimensions would be not only unique to “HIV” but to any other retrovirus seen using electron microscopy anywhere in the Universe. We wrote to Nature questioning this uncharacteristic lack of scientific rigor and suggested that, because of the importance of this matter, Nature could either seek clarification from the HIV experts or preferably arrange a scientific debate between the two sides adjudicated by disinterested scientists. In this manner the matter could be resolved once and for all. Our letter was rejected but we were told that Nature “will probably publish a correction”. Although the possibility cannot be excluded that such a correction has been made, so far we have not seen it. The front page of the International AIDS Society Newsletter, March 2007, is entitled “AIDS Denialists. This edition’s feature article examines the global impact of AIDS denialism”. About 75% of this page is occupied by a dazzlingly multi-coloured picture more appropriate for a discotheque than a scientific publication. Apparently it is meant to represent an electron micrograph of part of a cell with budding and cell free “HIV” particles. However, anybody who is familiar with electron micrographs will realise that the picture is a computer graphic. The picture has a caption which reads: “Image: HIV daughter cells bud on the surface of a T-cell”.41 Anyone with even rudimentary knowledge of medicine or biology knows that viruses are not cells and are gender free. The term “daughter cells” is absurd. On what “evidence-based science” is Bergman’s “overwhelming scientific consensus” based? In House of Numbers there is the following dialogue: Luc Montagnier: “I am a promoter of the role of co-factors in AIDS.” Harry Haverkos: “Well, co-factors just says that the cause of a disease is by more than one factor.” Joe Sonnabend: “Just simply being infected by HIV is not going to do it. You need certain co- factors.” Anthony Fauci MD, Director, National Institute of Allergy and Infectious Diseases: “Co-factors are not necessary.” Joe Sonnabend: “Dr. Fauci would say: HIV causes AIDS without the need of anything else. That is kind of ridiculous.” Anthony Fauci: “The data that indicate that any different type of infection like mycoplasma or something like that is a necessary co-factor, I believe those theories have been debunked.” Francoise Barre-Sinoussi PhD, Director, RRI, Institut Pasteur, France Nobel Laureate in Physiology or Medicine 2008: “We are almost convinced that there are also factors that are involved in the loss of CD-4 cells and we don’t know yet all the mechanics.” Jay A. Levy MD, Director, Laboratory for Tumor and AIDS Virus Research, UCSF: “How HIV depletes the T-cells so an individual advances to AIDS is probably due to multi-factorial elements. One is it will kill the cell eventually that it affects.” Joe Sonnabend: “What the fuck does he mean? I’m sorry, what does he mean that there are no co-factors. Where is he coming from? There’s co-factors for everything.” Robert Gallo: “Co-factor implies something specific. It really gets us off into tracks that are wandering.” Harry Haverkos: “Gallo isn’t going to change his mind when he’s probably 70 years plus now. He is going to remember things, we all remember things that are good for us and we forget the bad things...The co-factors are important to really understand how people get ill, why they get ill.” As far back as 1986 Gallo wrote: “the results revealed a cytopathogenic [cell killing] mechanism that may account for T4 cell depletion in AIDS patients and suggest how repeated antigenic stimulation by infectious agents such as malaria in Africa or by allogenic blood or semen, may be important determinants of the latency period in AIDS”.26 Is it possible that without such antigenic stimulation the latency period may well be infinite in “HIV” “infected” individuals? If antigenic stimulation is the absolutely necessary co-factor then “HIV” may be a co-factor which is absolutely unnecessary. Ten years ago researchers from the US (the Multicenter AIDS cohort study, University of California, the John Hopkins School of Public Health) and the UK wrote: “Our results underscore the conclusion that virus load and CD4+ T cell counts are not the only factors that influence the outcome of HIV-1 disease. Alternate pathogenic influences clearly carry more weight in advanced disease”.42 According to the dictionary consensus means “agreement in the judgment or opinion reached by a group as a whole”. Unless she has her own definition of “consensus”, even Bergman would have to agree that the “evidence-based science” proves there is barely any consensus amongst “HIV”/AIDS experts on anything. Bergman claims the “HIV” experts were deceived by Leung, he “cut up their words and edited them to make it appear as if there is no consensus among experts about the nature of HIV and the disease syndrome it causes, known as AIDS”. The fact is Leung did no such thing. The “HIV” experts gave an honest account of their various opinions and their words, which were not “cut up”, reveal what they apparently would rather deny - there is no consensus. Bergman: “HIV...is the cause of AIDS” The HIV theory of AIDS was put forward to account for two diseases in gay men, Kaposi’s sarcoma (KS) and Pneumocystis carinii pneumonia (PCP). By 1988 researchers from the Walter Reed Army Institute of Research stated: “in our system the presence of opportunistic infection is a criterion for the diagnosis of AIDS, but the presence of Kaposi’s sarcoma is omitted because the cancer is not caused by immune-suppression”.43 In 1990 Friedman-Kein published “evidence-based science” confirming the fact that in some homosexual men KS can occur in the absence of both immune deficiency and “HIV”.44 Since then, “HIV” experts have accepted that “HIV” is neither the direct nor the indirect cause of KS. Yet KS, not caused by “HIV”, remains an indicator disease of a syndrome caused by “HIV”. Another example of AIDS “evidence-based science”? For Bergman’s interest, in 1988 the Perth Group paper45 arguing that HIV does not cause Kaposi’s sarcoma was thrice rejected by the Medical Journal of Australia on the advice of an “established expert”. The reviewer stated, “The author tries to argue that Kaposi’s sarcoma cannot be caused by HIV infection, and that therefore AIDS is not due to HIV infection. The arguments put forward by the author are quite unsatisfactory, and are not supported by even a desultory reading of the literature quoted. In addition, the author fails to examine the body of epidemiological, immunological and cellular literature concerning the pathology, pathogenesis and clinical associations of this fascinating manifestation of HIV infection”. Yet this is the very “epidemiological, immunological and cellular literature” which eventually led all the “established experts” to accept that “this fascinating manifestation of HIV infection”, is not caused by HIV infection. This as good an example as any that “AIDSTruth” is not truth until AIDS experts say it is. In 1995 Gallo stated: “The first thing I can tell you is that we’ve been able to regularly culture from Kaposi’s tumors what pathologists say is a tumor cell. We asked: What is the role of HIV in all this? And we found that inflammatory cytokines ... were the very likely initiatory events in creating this cell. We said, “Oh, the role of HIV is likely to be in increasing these inflammatory cytokines.” But we have learned – this should be of interest to everybody that isn’t completely married to HIV – that the inflammatory cytokines are reportedly increased in gay men even without HIV infection. Inflammatory cytokines are usually promoted by immune activation, not by immune suppression. So here was a paradox....So the inflammatory cytokines may be increased by HIV, but I wish I knew what else was increasing them before a gay man was ever infected with HIV. Maybe it’s nitric oxide, maybe it’s a sexually transmitted virus, maybe it’s all of them, maybe it has to do with rimming because it’s immune stimulation with non-specific infections”46 (emphasis added). (As mentioned, contrary to Bergman’s “evidence-based science”, KS, a disease not caused directly or indirectly by “HIV”, still remains an AIDS indicator disease). In 2006 three prominent HIV/AIDS experts from the US, including Clifford Lane from the Division of Clinical Research and Laboratory of Immunoregulation, National Institute of Allergy and Infectious Diseases, Bethesda, commented on the Rodriguez 2006 JAMA paper.47 “The findings presented by Rodríguez et al provide support to those who favor nonvirological mechanisms as the predominant cause of CD4 cell loss; however, these data should be interpreted with caution, and the issue of a single viral load as a prognostic marker should be separated from the role of viral replication in HIV pathogenesis”. In other words, the AIDS “evidence-based science” appears to be sliding in the dissident direction. Regarding the role of viral replication in AIDS David Cooper, Director of the National Centre in HIV Epidemiology and Clinical Research, University of New South Wales, Sydney, wrote: “The major findings are that, despite improved initial HIV virological control (percentage <500 copies per mL at 6 months increased from 58% in 1995–96 to 83% in 2002–03), there were no significant improvements in early immunological response as measured by CD4-lymphocyte count, no reduction in all-cause mortality, and a significant increase in combined AIDS/AIDS-related death risk in more recent years...somewhat paradoxical...results”.48 Nonetheless, such paradoxical findings, yet more “evidence-based science” at odds with the HIV theory of AIDS, did not shake any belief in the “incontrovertible evidence”. In fact these results were reported as “success”. Paradoxical scientific theories require revision. Obviously “denial” is not the prerogative of “AIDS denialists”. In 1985 Montagnier stated “This [clinical AID] syndrome occurs in a minority of infected persons, who generally have in common a past of antigenic stimulation and of immune depression before LAV [HIV] infection”.49 That is, at the beginning of the “HIV” era Montagnier recognised that in the AIDS risk groups AID appears before HIV infection. He is still saying it. In a talk he gave to the European Parliament, 8th December 2003, Montagnier said the cause of the ‘‘clinical phase of opportunist infections and cancers which result in death [AIDS]’’ is principally due to a decline in the numbers of T4 cells. The decline in T4 cells is due to their ‘‘propensity to die from apoptosis’’. In turn apoptosis is due to ‘‘potent oxidative stress’’. In regard to African patients he said that the oxidative stress ‘‘exists even in the non-infected individuals because of malnutrition’’.7 That is, the cause of AIDS is oxidation, not an infectious retrovirus. It is ironic that the discoverer of “HIV” thinks the “evidence-based science” supports our oxidative theory of AIDS put at the very beginning of the AIDS era. Even before “HIV”. In fact nowadays Montagnier is an apologist for our theory.4,8 Bergman: “...people knowledgeable about HIV are clear that HIV is a hard virus to get” If this is “a hard virus to get” how did millions of people get it in such a short interval? Why was it increasing exponentially in gay men in the US shortly after 1980? And why are the vast majority of “infected” people either US or African blacks? And only in certain countries in Africa? Bergman: HIV...is transmitted by the...sexual fluids of infected people There has never been any proof that “HIV” is transmitted by the “sexual fluids of infected people”. All the “proof” of sexual transmission is based on epidemiological studies which document the relationship between a positive antibody test (“infection”) and various sexual behaviours, in both gay men and heterosexuals. (Apparently, despite much “evidence-based science” to the contrary,50 “HIV” experts regard “HIV” antibodies in the blood as synonymous with infectious “HIV” particles in “sexual fluids of infected people”). We remind Bergman that sexually transmitted infections or diseases are transmitted bidirectionally. That is, from the active (semen donating) partner (heterosexual or gay male) to his passive (semen accepting) partner (male or female) and vice versa. Hence epidemiological “evidence-based” proof that HIV/AIDS an infectious disease must demonstrate beyond all reasonable doubt that both the passive and the active partner are at risk of developing a positive antibody test or AIDS. We further remind Bergman that the interpretation of epidemiological evidence in gay men is complicated by the fact that gay men commonly practise both active and passive sex. Thus, in order to determine the relationship between sexual contact and a positive antibody test in the active partner, epidemiologists must provide data on gay men who exclusively practise active sex. While there is ample evidence the passive partner is at risk of acquiring a positive antibody test or AIDS, there is no evidence the active partner is similarly afflicted. In fact, not only do the data show there is no increased risk for the active partner, there are no data that any active partner acquires a positive antibody test or AIDS from his or her passive sexual partner. Let Bergman cite one study to the contrary. Here we list the relevant evidence. Note: we, like epidemiologists, discount findings from cross-sectional studies. That is, studies where both partners are simultaneously found to be “HIV” positive. This type of study cannot prove sexual transmission and it is for this reason that epidemiologists resort to the much more difficult, time consuming and expensive prospective studies. It also must be stressed that in these studies epidemiologists rely on self-reported data on sexual activity and behaviours which, as epidemiologists themselves accept, are inherently problematic. This is an especially significant factor when interpreting the low numbers of “transmissions” universally reported in such studies. In regard to such fallibility, as far back as 1988 Padian and Donald Francis wrote: “Over the years, a constant theme in the AIDS field has emerged from groups working in settings as different as blood bank donor deferral and AIDS-case categorization. Every group has found that extracting sensitive risk-behaviour information is often difficult for even the most experienced interviewer”.51 In 2006 Maria Gallo from the CDC reported a study on self-reported sexual behaviour in 332 female sex workers. She tested the women for intravaginal, prostate specific antigen (PSA), a specific marker for semen exposure. “Among women who reported no sex or protected sex only within the past 48 hours, 21% and 39%, respectively, tested positive for PSA. Among those testing positive for PSA, no differences in PSA concentrations were found among those reporting no sex, protected sex only, or at least one unprotected act”. She commented, citing 12 supportive studies: “Self-reported data are used for informing policy, research, and funding decisions regarding STI/HIV and pregnancy prevention efforts. Participants might give inaccurate responses as a result of self-presentation or courtesy bias,7,17–19 imperfect recall,20–23 poor question comprehension,24 limited topical vocabulary, exaggeration resulting from social norms or to comply with study eligibility criteria, personal salience of the sexual event, or emotional responses to sensitive questions.25–27 The high level of misreported recent exposure to semen that we demonstrated substantiates that self-reports of unprotected sex cannot be assumed to be valid measures. Future STI/HIV and pregnancy prevention studies should establish the veracity of self-reported measures of sex and condom use or should use end points that do not rely on self-reported data”. Robert Gallo and his associates were among the first to study the relationship between sexual activity and the acquisition of a positive antibody test. In 1984 Gallo reported: “of eight different sex acts, seropositivity correlated only with receptive anal intercourse...and with manual stimulation of the subject’s rectum...and was inversely correlated with insertive anal intercourse”.52 It goes without saying that an inverse relationship is totally at odds with the existence of a sexually transmitted, infectious agent. In an updated study published in 1986 they wrote: “Data from this and previous studies have shown that receptive rectal intercourse...is an important risk factor for HTLV-III infection [HIV]...We found no evidence that other forms of sexual activity contributed to the risk”.53 By 1994 many epidemiological studies, including prospective studies, were conducted in gay men. Reviewing more than 20 such studies Caceres and van Griensven concluded: “the cited reports yield convincing evidence that unprotected anogenital receptive intercourse poses the highest risk for the sexual acquisition of HIV-1 infection...there is mounting epidemiological evidence for a small risk attached to orogenital receptive sex, biologic plausibility, credible case reports and some studies show a modest risk, detectable only with powerful designs;...no or no consistent risk of the acquisition of HIV-1 infection has been reported regarding insertive intercourse and oro-anal sex”.54 Unquestionably, the largest, longest, best designed and executed prospective study in gay men is the Multicenter AIDS Cohort study (MACS). The authors of this study showed that “receptive anal intercourse was the ONLY sexual practice shown to be independently associated with an increased risk of seroconversion to HIV in this study”.55 The same authors also reported: “...greater sexual activity [receptive anal intercourse] following establishment of HIV-1 infection leads to exposure to promoters or co-factors that augment (or DETERMINE) the rate of progression to AIDS” 56 (emphasis added). This finding is at odds with the general accepted view for sexually transmitted diseases, namely, a person needs to be infected only once with a microorganism in order to develop and die from that illness. However, there is evidence that semen itself (or another, non-infectious factor associated with passive anal sex) is the cause of both a positive test and AIDS. There have been only two longitudinal studies in heterosexuals: the European Study Group published by de Vincenzi and her colleagues57 and Nancy Padian’s58 in the USA. However, both studies included a cross-sectional component. In her cross-sectional studies de Vincenzi reported that sexual practices “other than anal intercourse...were not associated with infection of the partner”. In their four year prospective study the authors of the European Group claimed 4 men and 8 women became infected following sex with the seropositive partner. This study was criticised by other researchers including Stuart Brody. He questioned their conclusion by pointing out that “The problem of subjects’ lying (often euphemistically termed “social desirability responding”) about engaging in anal intercourse and intravenous drug use plagues most studies of behavioral risk factors for the transmission of HIV, and the study by de Vincenzi and colleagues is no exception. How was the absence of homosexual contact verified? How was the absence of anal intercourse among the women verified? If only 4 men and 6 women among the 121 couples inconsistently using condoms lied when they denied engaging in anal intercourse (or misreported the facts for other reasons), there would be no cases attributable to vaginal intercourse without a condom. At least this much lying should be expected. Before vaginal and anal intercourse are assigned comparable degrees of risk and condoms given the credit for saving lives, the alternative explanation that the disease is spread almost exclusively by anal and intravenous transmission must be more rigorously examined. Other investigators found that HIV infection in women was related to anal intercourse (especially among partners of bisexual men) and the number of exposures to the index patient, but not to condom use or the total number of sexual partners”.59 Responding, de Vincenzi wrote: “We agree with Dr Brody that our prospective analysis lacks statistical power to show an increased risk associated with anal intercourse. [That is, they could not exclude the possibility that the positive antibody tests were the result of anal and not vaginal intercourse.] Indeed, we found such an association in the cross-sectional analysis. However, from a public health point of view, no one should state that there is no risk of HIV transmission through vaginal sex, since the vast majority of cases of AIDS throughout the world are acquired in this manner”. It is significant that de Vincenzi admitted her evidence did not prove HIV is transmitted by penile-vaginal intercourse. Neither did she cite evidence to prove her claim “the vast majority of cases of AIDS throughout the world are acquired” by penile-vaginal transmission. Unquestionably, Padian’s study, which began in 1985, is the longest, largest, best designed and executed study ever conducted in heterosexuals. At the 1988 Amsterdam International AIDS Conference, Padian described her study as follows: “Objective. To examine the efficiency of heterosexual transmission of HIV [emphasis ours] and associated risk factors. Methods: We enrolled the opposite sex partners of individuals infected with HIV or diagnosed with AIDS or ARC throughout California. Participants were interviewed about their sexual practices and medical history; Laboratory tests for HIV and other co-factors were conducted, as were physical examinations...Results:...in multivariate analysis, only the practice of anal intercourse (p-.003) and non-white race (p-.013) were significantly associated with infection...We have also enrolled male partners of infected women. In spite of reported unprotected sexual intercourse (median number of sexual contacts = 399) none of the twenty male partners were infected”.60 See also Padian Endnote. As was the case in the European study, the Padian study was divided into two parts: cross- sectional and prospective. The first findings from the cross-sectional study were published in 1987, in a paper entitled: “Male-to-Female Transmission of Human Immunodeficiency Virus”: “Ninety-seven female sexual partners of 93 men infected with human immunodeficiency virus were studied...23% of the women were infected...Anal intercourse significantly discriminated between seronegative and seropositive women...The number of sexual contacts (whether vaginal, anal or oral, was significantly associated with infection...whereas general sexual activity (as measured by number of sexual partners [median 2,5 for seropositive; 4 for seronegative women] and number of sexually transmitted diseases) was not associated with HIV infection”.61 In 1991 Padian et al published yet another paper describing their findings from the cross- sectional part of their study, this time entitled “Female-to-Male Transmission of Human Immunodeficiency Virus”.62 They pointed out that “since 1985, we have been conducting a study of the heterosexual transmission of AIDS”, but by 1991 of 72 infected women, only the partner of one of them was found positive. However, for a number of reasons they could not say with certainty that the man was infected by his female partner...We cannot be absolutely certain that we correctly classified this case as female-to-male transmission...Of course, because we are relying on risk histories, the same caveats apply to classification of male-to-female cases of transmission as well”. By 1997 Padian and her colleagues described one more case of female- to-male transmission about which they were equally uncertain. Trying to explain the differences between their findings and that of others, who claimed high rates of female-to-male transmissions, they wrote: “studies may not have been adequately controlled for other confounding non-sexual routes of transmission such as risks associated with intravenous drug use. At first blush, cases that appear attributed to heterosexual transmission may, after in depth interviewing, actually be linked to other sources of risk”.58 In 1997 in a paper entitled “Heterosexual Transmission of Human Immunodeficiency Virus (HIV) in Northern California: Results from a Ten-year Study”, Padian and her colleagues published their findings in the prospective study. Describing this part of the study Padian and her colleagues wrote: “We followed 175 HIV-discordant couples over time for a total of approximately 282 couple-years of follow-up...The longest duration of follow-up was 12 visits (6 years). Table 3 summarises behaviour change over time, comparing behaviours of the entry visit with those reported at the last follow-up visit”. active partner acquires a positive antibody test or AIDS from his or her passive sexual partner. Let Bergman cite one study to the contrary. Here we list the relevant evidence. Note: we, like epidemiologists, discount findings from cross-sectional studies. That is, studies where both partners are simultaneously found to be “HIV” positive. This type of study cannot prove sexual transmission and it is for this reason that epidemiologists resort to the much more difficult, time consuming and expensive prospective studies. It also must be stressed that in these studies epidemiologists rely on self-reported data on sexual activity and behaviours which, as epidemiologists themselves accept, are inherently problematic. This is an especially significant factor when interpreting the low numbers of “transmissions” universally reported in such studies. 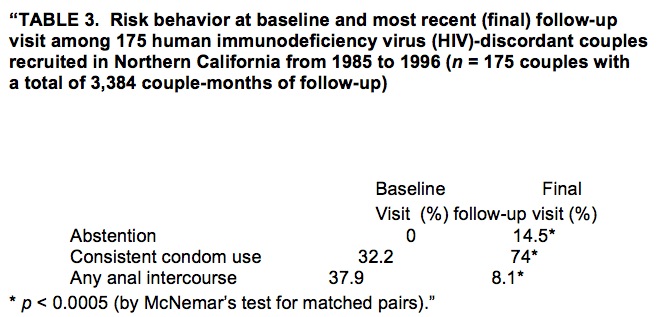 Despite an extraordinary effort educating her study subjects in safe sexual practices, Padian and her colleagues were not entirely successful, as can be seen from their Table 3. Furthermore, “approximately 97% of behaviour changes was reported between baseline and the first follow-up visit”. Yet, they “observed no seroconversion”, that is, no uninfected individual developing positive antibody test. Discussing the lack of sexual transmission, Padian and her associates wrote: “Nevertheless, the absence of seroincident infection over the course of the study cannot be entirely attributed to significant behaviour change. No transmission occurred among the 25% of couples who did not use condoms consistently at their last follow-up nor among the 47 couples who intermittently practiced unsafe sex during the entire duration of follow-up”.58 Hence Padian’s data prove “HIV” is not transmitted to the active partner.
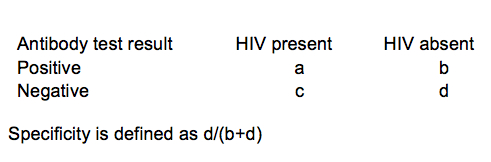
Padian consistently refuses to accept the “evidence-based science” conclusion of her own studies. She has even felt (or was) compelled to defend her “proof” of heterosexual transmission at AIDSTruth. Padian wants everyone to accept that, because she later decided to label her study as “behavioral interventions” to prevent HIV transmission, it is iniquitous to use her data to question proof of HIV transmission. Hence the title of her paper, Heterosexual transmission of human immunodeficiency virus (HIV) in Northern California: results from a ten-year study, remains a mystery. Why didn’t Padian choose a title reflecting what she later purported was its true nature? The fact is that in Padian’s study there were discordant heterosexual couples who continued to practise unsafe sex who nonetheless did not seroconvert to HIV. However, no scientist can claim the zero transmission rate observed in any couple was due to the success of “behavioral interventions” when, at the beginning of the study, approximately 70% of the couples were not practising safe sex, as were 26% at the completion, despite the many and constant “behavioral interventions”. Who or what was behind Padian’s emotional riposte in AIDSTruth: “Any attempt to refer to this or other of our publications and studies to bolster the fallacy that HIV is not transmitted heterosexually or homosexually is a gross misrepresentation of the facts and a travesty of the research that I have been involved in for more than a decade”? The evidence shows that it is Padian who is unwilling to face up to her own data. Bergman argues “The virus doesn’t care what you call it”. Even if “HIV” were a virus, whether a virus can “care” is a moot point. Be that as it may, a virus cannot “know” if it is participating in a study of “behavioral interventions” or transmission. Padian’s repackaging of her study illustrates her unwillingness to accept she was conducting an experiment in sexual transmission of “HIV” whether she likes it or not. And this study did not have any seroconversions. It is significant that in her AIDSTruth commentary Padian did not cite any of her own research as proof of heterosexual transmission. As with de Vincenzi, when it comes to citing proof of heterosexual transmission, Padian cites “everyone else”. Yet “everyone else” cites de Vincenzi and Padian. From the very beginning of the AIDS era, with few exceptions, there has been an unhealthy bias towards an infectious cause of a positive antibody test and AIDS. Scientists have not conducted research that might elucidate whether non-infectious factors, semen for example, may play the direct role in the development of a positive antibody test or AIDS. This is despite published data that, in the case of semen, it is both toxic and immunosuppressive. Virtually all epidemiological studies on sexual transmission illustrate this bias although it would have been a relatively simple matter to collect data to test whether the risk from passive anal sex is an infectious agent in semen or semen itself. For infectious agents the risk increases as the number of sexual partners. For semen itself or other non-infectious agents the risk increases as the number of episodes of sex. In case this distinction is not clear consider the following: The volume of the male ejaculate is reported to be 0.1-11 ml. Let us choose 5 ml as a typical quantity. Over a period of three months for example, a passive gay man could have a hundred partners, each once, which would expose him to 500 ml of semen. Or he could have 50 partners, four times, which would expose him to a litre of semen. That is, half as many partners could expose him to twice the dose of semen. If an infectious agent is the cause of a positive antibody test or AIDS then the hundred partners should pose more of a risk than the fifty partners. And vice versa. By performing such a study one could obtain data to distinguish between these possibilities. However, virtually no epidemiological study reports such data. What is reported is the number of (different) sexual partners, not the frequency of sex. There are two exceptions. One of the two studies is the 1987 Padian et al study61 where she found that “The number of sexual contacts (whether vaginal, anal or oral was significantly associated with infection...whereas general sexual activity (as measured by number of sexual partners...was not associated with HIV infection. The other exception is a study by Janet Nicholson published in the Annals of Internal Medicine. “In the year before testing, homosexual men who were seropositive tended to have a greater number of sexual partners (p = 0.009), more episodes of receptive anal intercourse (p < 0.001), and more frequent active (p < 0.001) and receptive (p = 0.023) insertion of hands into the rectum...The number of episodes of receptive anal intercourse per year was the variable most highly associated with HTLV-III/LAV seropositivity (F - 27. p < 0.001). After adjustment for this variable, no other variable was statistically significant”.63 In other words, in this study the number of episodes of receptive anal sex had more statistical significance than the number of partners. And in a subgroup of men analysed the quantity of semen was the only significant risk factor. Hence epidemiologists dismissed the early notion that semen may have been a cause of immunosuppression and AIDS to the point where evidence that could have added weight to this theory was not even collected. Yet these data should have been part of each and every study. Even when studies such as these are published, their “evidence-based science”, which does not support the existence of an AIDS causing, sexually transmitted agent, is ignored. In summary the only possible interpretation of the epidemiological data is that, unlike all the other sexually transmitted agents and diseases, “HIV” (a positive antibody test) or AIDS, is not bidirectionally transmitted. The passive partner acquires “HIV”/AIDS through sexual activity but cannot transmit either to the active partner. To use an analogy, AIDS is like pregnancy. It can be acquired by the passive partner but not transmitted to the active partner. The difference is that pregnancy can be acquired by a single act of vaginal intercourse while for the acquisition of a positive antibody test and AIDS, a high frequency of anal intercourse is necessary. In the case of “HIV”/AIDS either: (i) The active partner acquires “HIV” by means other than sex, and then transmits it to the passive partner; or (ii) The cause of AIDS and of the positive antibody test in the passive partner is not a retrovirus “HIV”. The most parsimonious explanation for the epidemiological data in both gay men and heterosexuals is that “HIV”/AIDS is not sexually transmitted because there is no infectious agent to transmit. Appreciation of this should have led “legitimate scientists, doctors and advocates” to question the “isolation” of “HIV” and a retroviral theory of AIDS. Bergman: HIV tests are extremely reliable, sensitive and specific...The ELISA or EIA test screens for the presence of HIV antibodies in blood or oral fluids... Because there is a small risk of a false positive, every HIV test is then confirmed with a Western Blot test. The two-test protocol is over 99.9% accurate (original emphasis) For a long time immunologists thought and taught that antibodies react only with the inducing antigen. Now they accept (but mostly ignore the obvious scientific consequences) that antibodies react with a plethora of other antigens.64-66 Hence it does not follow that an antigen/antibody reaction proves the antibody arose as a result of exposure to or infection with a particular antigen. The “accuracy” of a test encompasses several parameters including its specificity. Probably unknowingly, specificity is the test parameter of most interest to the patient because it raises the possibility that a positive result has a cause other than what Bergman would have us all believe. As Bergman states, specificity means “recognizing everyone who is a true negative, who doesn’t have the virus or whatever is tested for”. If a test is truly capable of “recognizing everyone who is a true negative [not infected]” then the test specificity is 100%. This is most often not the case – most tests are not 100% specific. The definition of specificity may be difficult to grasp because it involves two negatives, that is, the proportion of non-infected individuals who have negative tests. It is much easier to understand specificity in terms of the test being positive if and only if infection is present. In other words, a 100% specific test is never positive unless infection is present. All non-infected persons have a negative test. Every non-infected person who does have a positive test reduces the test specificity from its theoretical maximum. As usual, Bergman provides no evidence for her assertion but she does know specificity can only be determined by experiment. This experiment consists of testing a statistically significant (=large) number of individuals which must include (a) healthy individuals at no risk of AIDS; (b) people at risk of AIDS; (c) those suspected of being “infected” (AIDS patients); (d) sick individuals with clinical and laboratory abnormalities which closely resemble AIDS but are not AIDS. For example, since AIDS patients are oxidised and have hypergammaglobulinaemia, both highly typical of AIDS patients, so must the controls. Since the antibody test is claimed to diagnose HIV infection, for each individual the experiment must determine (a) the antibody test status; (b) the presence of absence of “HIV”. The method of determining (b) cannot be (a) because this would amount to a test evaluating itself and hence be scientifically invalid. Therefore method (b) must be a method which is independent of (a) and is usually known as the gold standard for the test. The gold standard is a crucial sine qua non and represents the tenet upon which rests the scientific proof of validity.67 No gold standard no validity. Hence, when the blood samples are obtained they are divided into two portions: one to test for antibodies, the other to isolate “HIV”. From these data the following table is then constructed where a, b, c and d are the numbers of individual categorised as per the table:
For example, if there are 500 individuals from whom “HIV” cannot be isolated and one such individual has a positive antibody test the specificity is 499/(1+499) = 99.8%. Nowhere in the 150,000 papers published to date on “HIV”/AIDS is there such a table. We challenge Bergman to produce even one instance of this table and post it at AIDSTruth. If she cannot she can only conclude there is no “evidence-based science” for her assertions. In the absence of these data the specificity of the “HIV” antibody tests is unknown. It may be 100% or it may be zero or any number in between. Since the “HIV” theory is solely based on a correlation between a positive antibody test and the clinical syndrome, in the absence of such data, there is no proof for this theory. If Bergman wants to seriously undermine the view of some of the “AIDS denialists” she could do no better than produce this table. Furthermore, if Bergman takes the time to examine the fundamental failure of “evidence-based science” to provide a gold standard for the antibody tests she will discover this is a direct consequence of the failure of HIV experts to purify “HIV”.12 13 Manufacturers of the “HIV” antibody test kits are fully aware of the need for a gold standard but, at the same time, accept it does not exist. Statements to this effect are regularly included as disclaimers in test kit packet inserts. For example, the Abbott Western blot antibody test kit insert: “At present there is no recognized standard for establishing the presence or absence of HIV-1 antibody in human blood”. Obviously biotechnology companies understand consequences that “HIV” experts deny. Some “HIV” experts themselves agree there is no gold standard: William Blattner: “One difficulty in assaying the specificity and sensitivity of human retroviruses [including HIV] is the absence of a final “gold standard”“. In the absence of gold standards for both HTLV-I and HIV-1, the true sensitivity and specificity for the detection of viral antibodies remains imprecise”.68 Philip Mortimer: “Diagnosis of HIV infection is based almost entirely on detection of antibodies to HIV, but there can be misleading cross-reactions between HIV proteins and antibodies formed against other proteins, and these may lead to false-positive reactions. Thus, it may be impossible to relate an antibody response specifically to HIV infection”69 (emphasis added). Elizabeth Dax (co-author with Niel Constantine) does not appear to understand the concept of a gold standard, much less the absolute need for a gold standard in establishing the specificity of an antibody test.25 There being no gold standard, “final” or otherwise, for the “HIV” antibody tests, Blattner, Gallo and their colleagues used AIDS as the gold standard. It is greatly ironic that Bergman herself knows this is wrong. She correctly defined specificity as “recognizing everyone who is a true negative, who doesn’t have the virus or whatever is tested for” (emphasis added). The “HIV” antibody tests are tests for “the virus” “HIV”, not AIDS. If a scientist uses AIDS as a gold standard he obtains the sensitivity and specificity of a test for AIDS, not “HIV”. Yet, the title of the Blattner and Gallo paper is “Screening Test for HTLV-III [“HIV”] (AIDS Agent) Antibodies”. This title is not justified by the data. The only time AIDS can be used as a gold standard for the “HIV” antibody tests instead of “HIV” is if there is proof that: (a) “HIV” causes AIDS and; (b) no other agent causes immune deficiency and the diseases which constitute the clinical AID syndrome. This is not the case now and never has been. Indeed, although the title of the Blattner and Gallo paper refers to “HIV” as the “AIDS Agent”, in the text they state: “HTLV-III has emerged as a LIKELY etiologic agent of the acquired immune deficiency syndrome (AIDS)”70 (emphasis added). In 1984 Gallo used the antibody test to obtain “clear-cut evidence” that “HIV” is the cause of AIDS while in the above paper he used the presence of AIDS as a gold standard to prove that the antibodies are specific to “HIV”. This is a circular argument in which “HIV” is bypassed. Furthermore, as already mentioned and as Bergman fully understands, if AIDS is used as a gold standard, since the vast majority of people who test positive do not have AIDS, the vast majority of positive tests are false positives. Niel Constantine, who appears in the House of Numbers, wrote a text book38 entitled “Retroviral testing and quality assurance. Essentials for laboratory diagnosis”. Addressing the determination of test parameters he wrote: “All serological confirmatory tests have guidelines or criteria that must be met to determine whether result fulfils the requirements to classify the sample as HIV positive, negative, or indeterminate. These criteria have been determined in two ways. First, manufacturers of test kits have predetermined the requirements for results based on studies of individuals who have been classified as positive or negative by other means (clinical status, culture etc.) (emphasis added)”. Constantine’s last sentence affirms the requirement for a gold standard: “...individuals who have been classified as positive or negative by other means”. The “other means”, that is, the gold standard is “clinical status, culture, etc”. If the clinical status “AIDS” is the gold standard for “HIV” then why do we need antibody tests? “Culture” means culturing a blood specimen from a patient and then adding an antibody that reacts with Montagnier’s p24 protein. This is nothing more than an antibody test where the unknown is reversed. That is, instead of adding unknown antibodies to a known antigens, a known antibody is added to an unknown antigen. However, no matter what is given, it is still the same antibody test and an antibody test cannot be its own gold standard. The Perth Group will award a prize to anyone who can provide a scientific definition of an “etc.” gold standard. So much for “evidence- based science”. Since to date nobody has proven the specificity of the antibody tests for “HIV” infection by the use of an “HIV” isolation gold standard, it is unreservedly valid to ask whether the antibodies that react with the test kit antigens are induced by factors or antigens that are not in any manner related to a putative retrovirus “HIV”. According to Constantine et al: “The best antigen preparations to detect established HIV infection are viral lysates because these contain native antigens from virtually all structural components of the virus”. “Viral lysates” is the material from the culture supernatant which in sucrose density gradients bands at the density of 1.1 6g/ml. The most important “viral proteins” used in the “HIV” antibody tests are p24, p32, p41, p120 and p160. However, as stated earlier, in the “viral lysates”, where Montagnier identified the “HIV” p24, there was only cellular debris, no retroviral particles. That is, according to the “evidence-based science”, p24 is a cellular protein. Also according to Constantine: “The gp160 molecule is a precursor, being subsequently cleaved to form gp120 and gp41...It has been demonstrated that the gp160 antigen on Western blots may actually be tetramers [X4] of the gp 41 antigen (and not the precursor env protein); this may occur during the disruption and electrophoresis procedures. Therefore, antibody reactivity to the gp160 antigen (and gp41) may actually represent reactivity to gp41 only. Also, the env specific antigen in the position of gp120 is in fact a mixture of the trimer [X3] of gp41 and true outer membrane protein gp120”. Hence there is no evidence that the p120 or p160 band on the Western blot contain any protein other than p41. According to Montagnier, p41 is the cellular protein actin and Bess et al have published data that all the “HIV” proteins with molecular weights higher than 30,000 (including p41) are all cellular proteins. In other words, none of the protein antigens from the “viral lysates” used in the “HIV” antibody test kits are viral. Rather they are all cellular proteins. Bergman admits that individuals who have autoimmune diseases but not AIDS may react in the “HIV” antibody tests. At present there is ample evidence that oxidised globulins behave as autoantibodies.71 Given that: 1. In the “HIV” antibody test kits the antigens are cellular.16 2. One of the most important characteristics of people with AIDS and those at risk of AIDS 3. AIDS patients and those at risk, as the Perth Group predicted in 1988, are oxidised. 4. Oxidised antibodies become “unmasked” autoantibodies.71 5. AIDS patients and those at risk have a plethora of antibodies that react with many it is very likely that a positive antibody test is a non-specific marker, similar to, for example, the erythrocyte sedimentation rate, that indicates a propensity for the development of particular diseases (AIDS) but devoid of any connection to a putative retrovirus “HIV”. Bergman’s claim that the “HIV” antibody tests are 99.9% specific is not shared by some of the best known “HIV” experts, including some who appeared in House of Numbers: Robin Weiss: “I don’t think the Western Blot is a useful diagnostic test; I don’t think it’s worth doing...You don’t need a Western Blot! And it’s become a dogma in HIV research that you need one ELISA followed by a western; you don’t. You need two different kinds of ELISAs made in two different formats”. Weiss’ recently expounded on these statements at the bogus House of Numbers website set up by Bergman. He claims he was discussing screening tests, not diagnostic tests. In “What interviewees say” Weiss states “In my recollection (I don't have a tape of the interview) Leung was pressing me about HIV antibody tests in reference to screening blood donations. When I said ‘I don't think the Western Blot is a useful diagnostic test; I don't think it's worth doing’, I was referring to relatively high throughput screening for blood banks, and in the mid 1980s”. In the House of Numbers it is quite clear Weiss is discussing diagnostic assays. The “dogma” “you need one ELISA followed by a western [blot] is not relevant to “relatively high throughput screening for blood banks”. Weiss also affirmed his opinion “You don’t need a Western blot!” as “ELISA tests made by two different manufacturers can also provide a confirmed result”. As far back as 1991 Philip Mortimer, Director, Sexually Transmitted and Blood Borne Virus Laboratory, United Kingdom, published a paper in Lancet entitled “The fallibility of the Western blot”: “Interpretation of these reactions is often difficult, even for experienced personnel....Interpretation of western blot patterns differs according to the observer and laboratory, and attempts to standardise western blotting by establishing interlaboratory guidelines for reading the strips have been met with only limited success. Manufacturers list their own criteria for interpreting western blots, as do the Centers for Disease Control (CDC) and at least five other US bodies. The World Health Organisation, which set criteria in 1988, revised them in 1990. Individual laboratories may add criteria of their own, and in a recent quality assessment exercise it was found that participating laboratories had developed eleven different sets of criteria to read western blots. Confusion of this sort must lead to errors”. Like Weiss, Mortimer concluded “Western blot detection of HIV antibodies began as, and should have remained, a research tool”.75 In “What interviewees say” Weiss concedes there are “doubts about the precision or reliability of tests that were devised as research tools in 1984”, which include the Western blot. Yet Weiss appears to forget that thousands of individuals were diagnosed with HIV using tests of such doubtful “precision and reliability”, including one test, the “confirmatory” Western blot, that “should have remained, a research tool”. Now, Weiss assures us, there are “mass produced commercial tests, which had to go through extensive quality control before they were marketed or used in clinics and blood banks”. Western blot tests may be mass produced but the problems enumerated by Mortimer still remain. More importantly, no antibody test, whether mass produced or produced in a research laboratory, should be introduced into clinical practice without proof of its specificity. Weiss compares “HIV” serology 1984 and now with “Roentgen's original fuzzy X- ray pictures” and today’s “radiological imaging systems for hospital diagnosis”. The reality is there has never been “a picture” of the Western blot, “fuzzy” much less “non-fuzzy”. Robert Redfield MD, Director, Clinical Care and Research Institute of Human Virology: “We have a group now, about 40 patients that have no detectable virus in their body but they’re not being treated. So the first question is, ‘are they really being infected?’” *Leung: “So the Western Blot could have false positives?” Robert Redfield: “No, the Western Blot was negative too. But they were told they were positive by a lab, yes, which misread the Western Blot. *Leung: “Heavyweight champion Tommy Morrison tested positive in 1996. Eleven years later, in 2007, he tested negative multiple times, allowing him to return to the ring.” Harold Jaffe: “There’s constant discussion in the community of people who do diagnostic testing and the blood bankers about how to read these tests.” *Leung: “When you’re looking at this, this western blot, how do you determine whether it’s a positive?” Claudia Kucherer: “You need a certain number of bands being present. It depends a little bit on the producer of the test.” *Leung: “It depends on the manufacturer.” Claudia Kucherer: “Yeah.” *Leung: “Is there a different criteria for what might be a positive?” Claudia Kucherer: “Yeah. Yes. There are different criteria from the manufacturer, thank you for the word, and also there are guidelines from the WHO and UNAIDS.” James Curran: “HIV infection is diagnosed with rather, now, routine laboratory tests for which there are criteria for diagnosis established by the manufacturer, FDA.” *Leung: “Claudia showed me the package insert that comes with the western blot. It contains eight different sets of criteria for diagnosis HIV infection.” *Leung: “Since a false positive looks like a true positive how can you ever distinguish whether it’s truly a positive or negative?” Fassil Keteman, MS: Director of Clinical Trial, Institute of Human Virology: ”Well that’s a great question, it’s going to be very hard to determine a false positive.” Max Essex: “ELISA and WB results should be interpreted with caution when screening individuals infected with M. tuberculosis or other mycobacterial species...ELISA and WB may not be sufficient for HIV diagnosis in AIDS-endemic areas of Central Africa where the prevalence of mycobacterial diseases is quite high”.72 Constantine et al: “The purpose of serologic confirmatory tests is to rule out false-positive results by screening tests, not to confirm that a person is unequivocally infected with HIV”.38 Since the antibody tests are the “proof” that “HIV”/AIDS has afflicted and killed millions of people around the world but their specificity for “HIV” infection has never been determined, how it is possible to measure the harm done by all the “legitimate scientists, doctors and advocates”? Bergman: “...the current generation of antiretroviral drugs for HIV are effective” There are NO randomised, double blind, placebo controlled trials of ARVs. So after 28 years of AIDS there is still no Level 1 evidence on the effects of ARVs on health or survival. So much for “evidence-based” AIDS medicine. Even if patients do improve while taking ARVs, as witnessed for example by Joe Sonnabend, this does not prove these drugs are “antiviral” or that HIV exists and causes AIDS. A decade ago Giorgi wrote: “Of interest, if antiretroviral drug use did affect survival in our study, the drugs did not seem to operate by effect on CD4 cell count or virus load, since these values were not different in the 2 groups...Our finding that virus burden did not associate with survival time is unlikely to be due to technical factors”.42 The “two groups” were the long and short term survivors. According to Mary Ann Chiasson, assistant commissioner of the New York City Department of Health, improvements in AIDS therapies may be “linked more closely to an increase in federal funding in 1994 for AIDS patients, which led to better prevention and treatment of opportunistic infections”.76 Indeed, in the same year, Zaunders et al presented unequivocal scientific evidence that any benefits of HAART cannot be the result of an “anti-HIV” effect.77 Bergman: The makers of “House of Numbers” deceived legitimate HIV researchers, infectious disease doctors, and AIDS activists and philanthropists to get interviews with them.. Bergman paints a sorry picture of gullible yet highly intelligent people. These scientists typically work in large institutions, run large departments as well as face the annual gauntlet of funding applications, with all the attendant politics. Bergman leads us to think they were so naïve they did not know journalists seek all views on a subject. Perhaps the truth is they saw Leung as a young man keen to find out as much as he could and most were more than willing to share their knowledge. In their eagerness they simply did not conceive Leung would seek anyone else’s point of view. In spite of the fact such views have been published in peer-reviewed scientific journals and are on the internet. The deception is not Leung’s. Leung was just doing his job. Bergman: These facts have been established in laboratories, clinically, and by epidemiology, and published in tens of thousands of peer-reviewed publications. More catechism without evidence. Name a scientific paper that proves HIV exists. Name a paper that proves “HIV” DNA and RNA are unique. Name a paper that proves the antibody tests are specific. Name a paper that proves HIV kills T4 cells. Name a paper that proves low T4 cells is necessary and sufficient to cause AIDS. Name a paper that proves ARVs prolong life. Explain the HAART “paradox”, as stated by HIV expert David Cooper in his commentary on the paper by May et al, Lancet 2006; 368: 451–58. Bergman: We have much still to learn about HIV and AIDS, and some scientists don’t like each other, but no legitimate, qualified scientist or doctor questions the existence or consequences of the virus. The vast majority of scientists and “qualified” doctors (are there unqualified doctors?) could not defend the HIV theory of AIDS. Most doctors cannot explain a Western blot test. Bergman seems to think adjectives such as “legitimate” and “qualified”, applied to scientists, are all you need to prove HIV exists and causes AIDS. Bergman: Differences in diagnostic criteria by region reflect lack of access to HIV testing technologies and different clinical approaches: specifically, most African countries’ health systems cannot afford HIV testing. That doesn’t mean that HIV doesn’t exist or that poverty causes AIDS. Where HIV tests are not available, an AIDS diagnosis obviously cannot include HIV status as an element of an AIDS diagnosis, so the diagnosis is based on the presence of opportunistic infections that would only afflict a person with a compromised immune system. It is ridiculous to defend a diagnosis of AIDS, caused by HIV, without evidence of HIV infection. Would Bergman accept a diagnosis of syphilis without a test for Treponema pallidum? Would she accept a diagnosis of AIDS or HIV infection in herself or a relative without an “HIV” test? The fact that testing is not available does not alter this fact. Doesn’t Bergman know that “immune deficiency” has been present in Africa for centuries before AIDS? Did all the factors contributing to African “non-HIV” immune deficiency suddenly disappear in the 1980s to make way for HIV? Does she know that for many years extra-pulmonary TB was AIDS defining but pulmonary TB was not? Did “HIV” know how to cause immune deficiency in ways such that AIDS developed in some individuals but not others when both became infected with Mycobacterium tuberculosis? How does Bergman explain Gallo’s discovery of HIV infection in 70% of a sample of healthy Ugandan children in 1972?78 How did this happen and why was there no AIDS in Uganda in 1972? Bergman: *Val Turner MD Perth Australia: “It’s ludicrous that you can be positive in one country and not positive in another.” This is an artifact of test design and does mean HIV infection differs from one country to another. This statement loses Bergman or whoever is advising her all credibility. Bergman appears quite comfortable with the fact that diagnostic criteria for the virus that “gradually destroys the human immune system, resulting in AIDS, a syndrome manifesting in various diseases...and ultimately death in people with advanced HIV disease” varies by laboratory, institution and country. This variation refers to the designated and number of bands required for a positive Western blot “confirmatory” antibody test. For example, a p24 and p41 band is positive in parts of the US but not in Australia or Africa. In Australia and Africa p24 and p41 would be reported “indeterminate”. According to Fauci, most indeterminates are not infected with HIV.79 This is indeed ludicrous. “HIV” antibody tests are tests for “HIV” infection. A person is either infected or not - no matter where he or she stands, sleeps or travels. And no matter where tested. Infection does not vary with latitude and longitude. Hence, no matter where a person is tested and regardless of which criteria are used, the person should receive the same diagnosis. Infected or not infected. A patient with a heart attack or cancer gets the same diagnosis in NYC, Australia and Africa. Not so for “HIV”.80 For Bergman’s interest, in 199481 we asked the Head of the Australian National Serology Reference Laboratory for proof of the Australian criteria for a “confirmatory” Western blot. Her response avoided answering the question but nowhere did she even suggest it was “an artifact of test design”. Perhaps Bergman could enlighten her. http://www.theperthgroup.com/SCIPAPERS/VFTDax.pdf Padian Endnote REFERENCES
1. Judson H. The great betrayal: Fraud in science. 1 ed. Orlando: Harcourt, 2004. 2. Papadopulos-Eleopulos E. Reappraisal of AIDS: Is the oxidation caused by the risk factors the 3. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM. Oxidative stress, HIV and AIDS. Res Immunol 1992;143:145-8. 4. Papadopulos-Eleopulos E. A Mitotic Theory. J Theor Biol 1982;96:741-758. http://www.theperthgroup.com/EPE/MitoticTheory.pdf 5. Piedimonte G, Guetard D, Magnani M, Corsi D, Picerno I, Spataro P, et al. Oxidative protein damage and degradation in lymphocytes from patients infected with human immunodeficiency virus. J Infect Dis 1997;176:655-64. 6. Montagnier L. Virus. New York: WW Norton & Company Inc, 2000. 7. Montagnier L. Apports de la recherche dans la lutte contra le Sida en Afrique. In: Pietteur M, 8. Papadopulos-Eleopulos E, Page BA, Causer D, Turner VF, Papadimitriou JM, Alfonso H. 9. Levy JA, Fraenkel-Conrat H, Owens RA. Virology. 3rd ed. London: Prentice-Hall, 1994. 10. White DO, Fenner FJ. Medical Virology. 4th ed. San Diego: Academic Press, 1986. 11. Papadopulos-Eleopulos E, Turner V, Weiss R. Email debate with Professor Robin Weiss on 12. Bess JW, Gorelick RJ, Bosche WJ, Henderson LE, Arthur LO. Microvesicles are a source of contaminating cellular proteins found in purified HIV-1 preparations. Virol 1997;230:134- 13. Gluschankof P, Mondor I, Gelderblom HR, Sattentau QJ. Cell membrane vesicles are a major 14. Barré-Sinoussi F, Chermann JC, Rey F, Nugeyre MT, Chamaret S, Gruest J, et al. Isolation of 15. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Page BA, Causer D, Alfonso H, et 16. Papadopulos-Eleopopulos E. No proof for the existence of HIV-evidence in chief at the 17. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Page BAP, Causer D. A critical analysis of Montagnier's 1983 "seminal" Science paper. http://theperthgroup.com/Nobel/Montagnier1983Paper.pdf 18. Sinoussi F, Mendiola L, Chermann JC. Purification and partial differentiation of the particles of murine sarcoma virus (M. MSV) according to their sedimentation rates in sucrose density gradients. Spectra 1973;4:237-243. http://theperthgroup.com/OTHER/Spectra.html 19. Pachacz M. No need to be phased. Shares 2001;6:28-32. http://www.theperthgroup.com/POPPAPERS/SharesMagazine2001.pdf 20. Panem S. C Type Virus Expression in the Placenta. Curr Top Pathol 1979;66:175-189. 21. Dourmashkin RR, Bucher D, Oxford JS. Small virus-like particles bud from the cell 22. Tahi D. Did Luc Montagnier discover HIV? Text of video interview with Professor Luc Montagnier at the Pasteur Institute July 18th 1997. Continuum 1998;5:30-34. http://www.virusmyth.net/aids/data/dtinterviewlm.htm http://www.altheal.org/continuum/Vol5no2.pdf 23. Gallo RC, Sarin PS, Kramarsky B, Salahuddin Z, Markham P, Popovic M. First isolation of HTLV-III. Nature 1986;321:119. 24. Gallo RC, Wong-Staal F, Reitz M, Gallagher RE, Miller N, Gillespie DH. Some evidence for infectious type-C virus in humans. In: Balimore D, Huang AS, Fox CF, editors. Animal Virology. New York: Academic Press Inc., 1976:385-405. 25. R v PARENZEE [2007] SACS 143. http://www.garlan.org/Cases/Parenzee/ 26. Zagury D, Bernard J, Leonard R, Cheynier R, Feldman M, Sarin PS, et al. Long-Term 27. Gallo RC, Montagnier L. The discovery of HIV as the cause of AIDS. N Engl J Med 28. Gallo RC, Salahuddin SZ, Popovic M, Shearer GM, Kaplan M, Haynes BF, et al. Frequent Detection and Isolation of Cytopathic Retroviruses (HTLV-III) from Patients with AIDS and at Risk for AIDS. Science 1984;224:500-503. 29. Goudsmit J. Viral Sex-The Nature of AIDS. New York: Oxford University Press, 1997. 30. Vahlne A. A historical reflection on the discovery of human retroviruses. Retrovirology 31. Gallo RC, Montagnier L. AIDS in 1988. Sci Am 1988;259:24-32. 32. Sarngadharan MG, Allaudeen HS, Gallo RC. Reverse transcriptase of RNA tumor viruses and 33. Gallo RC, Sarin PS, Wu AM. On the nature of the Nucleic Acids and RNA Dependent DNA 34. Varmus H. Retroviruses. Science 1988;240:1427-35. 35. Varmus H. Reverse Transcription. Sci Am 1987;257:48-54. 3 6. Gonda MA, Wong-Staal F, Gallo RC, Clements JE, Narayan O, Gilden RV. Sequence 37. Papadopulos-Eleopopulos E, Turner V, Papadimitriou J, Causer D. Are Montagnier's particles are retrovirus? http://www.theperthgroup.com/Nobel/MontagnierEMNobel.pdf 38. Constantine NT, Saville R, Dax E. Retroviral testing and quality assurance. Essentials for laboratory diagnosis. Halifax: MedMira Laboratories, 2005. 39. Layne SP, Merges MJ, Dembo M, Spouge JL, Conley SR, Moore JP, et al. Factors underlying spontaneous inactivation and susceptibility to neutralization of human immunodeficiency virus. Virol 1992;189:695-714. 40. Kuznetsov YG, Victoria JG, Robinson WE, Jr., McPherson A. Atomic force microscopy investigation of human immunodeficiency virus (HIV) and HIV-infected lymphocytes. J Virol 2003;77:11896-909. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=14581526 41. Anonymous. AIDS Denialists. International AIDS Society Newsletter 2007:1. http://www.iasociety.org/Web/WebContent/File/Old/PDF/1293.pdf 42. Giorgi JV, Hultin LE, McKeating JA, Johnson TD, Owens B, Jacobson LP, et al. Shorter survival in advanced human immunodeficiency virus type 1 infection is more closely associated with T lymphocyte activation than with plasma virus burden or virus chemokine coreceptor usage. J Infect Dis 1999;179:859-70. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=10068581 43. Redfield RR, Burke DS. HIV Infection:The clinical Picture. Scientific American 1988;259:70- 78. 44. Friedman-Kien AE, Saltzman BR, Cao YZ, Nestor MS, Mirabile M, Li JJ, et al. Kaposi's sarcoma in HIV-negative homosexual men. Lancet 1990;335:168-9. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=1967458 45. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM. Kaposi's sarcoma and HIV. Med Hypotheses 1992;39:22-9. http://www.theperthgroup.com/SCIPAPERS/ks.html 46. Lauritsen J. NIDA Meeting Calls for Research into the Poppers-Kaposi's Sarcoma Connection. The New York Native 1994. www.virusmyth.net/aids/data/jlpoppers.htm 47. Rodriguez B, Sethi AK, Cheruvu VK, Mackay W, Bosch RJ, Kitahata M, et al. Predictive value of plasma HIV RNA level on rate of CD4 T-cell decline in untreated HIV infection. JAMA 2006;296:1498-506. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=17003398 48. Dore G, Cooper D. HAART's first decade: success brings further challenges. Lancet 2006;368:427-428. 49. Montagnier L. Lymphadenopathy-Associated Virus: From Molecular Biology to Pathogenicity. Ann Int Med 1985;103:689-693. 50. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Alfonso H, Page BAP, Causer D, et al. Mother to Child Transmission of HIV and its Prevention with ATZ and Nevirapine. Perth: The Perth Group, 2001. 51. Padian N, Francis D. Preventing the heterosexual spread of AIDS. JAMA 1988;260:1879-81. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=3418846 52. Goedert JJ, Sarngadharan MG, Biggar RJ, Weiss SH, Winn DM, Grossman RJ, et al. Determinants of retrovirus (HTLV-III) antibody and immunodeficiency conditions in homosexual men. Lancet 1984;2:711-6. 53. Redfield RR, Wright DC, Markham PD, Salahuddin SZ, Sarngadharan MG, Gallo RC. Female-to-male transmission of HTLV-III. JAMA 1986;255:1703-6. 54. Caceres CF, van Griensven GJP. Male homosexual transmission of HIV-1. AIDS 1994;8:1051-1061. 55. Kingsley LA, Kaslow R, Rinaldo CR, Detre K, Odaka N, VanRaden M, et al. Risk factors for seroconversion to human immunodeficiency virus among male homosexuals. Lancet 1987;i:345-348. 56. Phair J, Jacobson L, Detals R, Rinaldo C, Saah A, Schrager L, et al. Acquired Immune Deficiency Syndrome Occuring Within 5 Years of Infection with Human Immunodeficiency Virus Type-1: The Multicenter AIDS Cohort Study. J Acquir Immun Defic Syndr 1992;5:490-496. 57. de Vincenzi I. A longitudinal study of human immunodeficiency virus transmission by heterosexual partners on Heterosexual Transmission of HIV. N Engl J Med 1994;331:341-6. 58. Padian NS, Shiboski SC, Glass SO, Vittinghoff E. Heterosexual transmission of human immunodeficiency virus (HIV) in northern California: results from a ten-year study. Am J Epidemiol 1997;146:350-357. 59. Brody S. Heterosexual transmission of HIV. N Engl J Med 1994;331:1718; author reply 1718- 9. 60. Padian N, Glass S, Marquis L, Wiley J, Winkelstein W. Heterosexual transmission of HIV in California: Results from a heterosexual partner's study. IVth International Conference on AIDS; 1988; Stockholm. 61. Padian N, Marquis L, Francis DP, Anderson RE, Rutherford GW, O'Malley PM, et al. Male-to- female transmission of human immunodeficiency virus. JAMA 1987;258:788-90. 62. Padian NS, Shiboski SC, Jewell NP. Female-to-male transmission of human immunodeficiency virus. JAMA 1991;266:1664-1667. 63. Nicholson JK, McDougal JS, Jaffe HW, Spira TJ, Kennedy MS, Jones BM, et al. Exposure to human T-lymphotropic virus type III/lymphadenopathy-associated virus and immunologic abnormalities in asymptomatic homosexual men. Ann Int Med 1985;103:37-42. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=2988389 64. Kramer A, Keitel T, Winkler K, Stocklein W, Hohne W, Schneider-Mergener J. Molecular basis for the binding promiscuity of an anti-p24 (HIV-1) monoclonal antibody. Cell 1997;91:799- 809. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=9413989 65. Predki PF, Mattoon D, Bangham R, Schweitzer B, Michaud G. Protein microarrays: a new tool for profiling antibody cross-reactivity. Hum Antibodies 2005;14:7-15. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=16424595 66. Marchalonis JJ, Adelman MK, Robey IF, Schluter SF, Edmundson AB. Exquisite specificity and peptide epitope recognition promiscuity, properties shared by antibodies from sharks to humans. Journal of Molecular Recognition 2001;14:110-21. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=11301481 67. Griner PF, Mayewski RJ, Mushlin AI. Selection and interpretation of diagnostic tests and procedures. Ann Int Med 1981;94:559-563. 68. Blattner WA. Retroviruses. In: Evans AS, editor. Viral infections of humans. 3rd ed. New York: Plenum Medical Book Company, 1989:545-592. 69. Mortimer PP. The AIDS virus and the AIDS test. Med Internat 1988;56:2334-2339. 70. Weiss SH, Goedert JJ, Sarngadharan MG, Bodner AJ, Gallo RC, Blattner WA. Screening test 71. McIntyre JA, Wagenknecht DR, Faulk WP. Autoantibodies unmasked by redox reactions. Journal of Autoimmunity 2005;24:311-7. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=15927793 72. Kashala O, Marlink R, Ilunga M, Diese M, Gormus B, Xu K, et al. Infection with human immunodeficiency virus type 1 (HIV-1) and human T cell lymphotropic viruses among leprosy patients and contacts: correlation between HIV-1 cross-reactivity and antibodies to lipoarabinomannan. J Infect Dis 1994;169:296-304. 73. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Causer D, Page BA. HIV antibody tests and viral load--more unanswered questions and a further plea for clarification. Curr Med Res Opinion 1998;14:185-6. http://www.theperthgroup.com/SCIPAPERS/furtherplea.html 74. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM, Stewart G, Causer D. HIV antibodies: further questions and a plea for clarification. Curr Med Res Opinion 1997;13:627-34. http://www.theperthgroup.com/SCIPAPERS/epcurmedres97.html 75. Mortimer P. The fallability of HIV western blot. Lancet 1991;337:286-287. 76. Cohen J. Advances painted in shades of gray at a D.C. conference. Science 1997;275:615-6. 77. Papadopulos-Eleopopulos E, Turner VF, Papadimitriou JM, Alfonso H, Page B, Causer D. 78. Saxinger WC, Levine PH, Dean AG, de The G, Lange-Wantzin G, Moghissi J, et al. Evidence for exposure to HTLV-III in Uganda before 1973. Science 1985;227:1036-8. 79. Fauci AS, Lane HC. Human Immunodeficiency Virus (HIV) Disease. In: Isselbacher AS, Braunwald E, Wilson JD, Martin JB, Fauci AS, Kasper DL, editors. Harrinson's Principles of Internal Medicine. New York: McGraw Hill Inc., 1993. 80. Papadopulos-Eleopulos E, Turner VF, Papadimitriou JM. Is a positive Western blot proof of HIV infection? Biotechnology 1993;11:696-707. http://www.theperthgroup.com/SCIPAPERS/biotek8.html 81. Turner VF. The HIV Western blot. Med J Aust 1994;160:807-808. http://www.theperthgroup.com/SCIPAPERS/VFTDax.pdf 82. Carlson JR, Bryant ML, Hinrichs SH, Yamamoto JK, Levy NB, Yee J, et al. AIDS serology testing in low- and high-risk groups. JAMA 1985;253:3405-8. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation &list_uids=2987558 |